
How staff training reduces Legionella risk in facilities
- 2 days ago
- 10 min read
Many facilities managers assume that a completed risk assessment and a written scheme of control are enough to keep their water systems safe. They are not. Real-world Legionella outbreaks, including several investigated by the UK Health Security Agency in recent years, consistently reveal the same root cause: staff who did not know what to do, when to act, or how to escalate. This article walks you through a practical framework for building genuine competence in your team, covering legal requirements, role-specific training, healthcare-specific mandates, and how to handle the edge cases that written procedures rarely anticipate.
Table of Contents
Key Takeaways
Point | Details |
Training prevents paperwork-only compliance | Real risk reduction depends on competent staff, not just written schemes. |
Role-based frameworks are vital | Training matched to each staff position secures operational safety and legal compliance. |
Refreshers and evaluations matter | Regular retraining and competence assessments ensure lasting effectiveness. |
Edge case preparedness | Staff training prepares facilities for unusual risks and rapid outbreak response. |
What is Legionella risk and why paperwork isn’t enough
Legionella bacteria thrive in water systems where temperatures sit between 20°C and 45°C, water is stagnant, and nutrients such as rust, scale, or biofilm are present. In commercial and healthcare facilities, the risk is particularly acute in cooling towers, hot and cold water distribution systems, spa pools, and any outlet that sees intermittent use. A complex hospital site or a large commercial building can have hundreds of such risk points, all requiring consistent monitoring and control.
The legal framework in England and Wales is clear. The Health and Safety at Work etc. Act 1974 places a duty on employers and those responsible for premises. The Approved Code of Practice, ACOP L8, and the associated HSG274 guidance documents set out exactly how that duty must be discharged. In healthcare, NHS England’s Health Technical Memorandum HTM 04-01 adds a further layer of specific requirements for water safety.
What these documents mandate is not simply a paper trail. They require a responsible person who is competent, a written scheme of control that reflects the actual system, and crucially, staff who are trained to implement that scheme reliably. The gap between what is written and what actually happens on the ground is where most compliance failures occur.
Documented control | Operational reality without training |
Weekly flushing schedules recorded | Staff flush outlets inconsistently or skip low-traffic areas |
Temperature monitoring logs signed | Readings taken incorrectly or out-of-range values not escalated |
Chemical dosing programme in place | Dosing adjusted without authorisation after system changes |
Cooling tower blowdown procedure written | Contractor carries out blowdown without notification to responsible person |
Thermostatic mixing valve (TMV) service records | TMV serviced on incorrect intervals because technician was not briefed |
As training for Legionella awareness specialists consistently find, the table above is not theoretical. These scenarios appear in audit findings across commercial and healthcare sites every year. The written scheme exists, the paperwork is signed, and yet the control measures are not being carried out as intended.
“Staff training reduces Legionella risk mainly by building competence to identify hazards, operate control measures as intended, and respond to deviations, so water hygiene controls are actually carried out, not just documented.”
This distinction matters enormously. A risk assessment is a snapshot of hazard potential; training is what converts that snapshot into daily, reliable action. For more on interpreting compliance requirements in context, the regulatory insights for compliance section of our website provides practical guidance for facilities teams.
Having outlined why written schemes often fail in isolation, let’s examine how staff training transforms compliance into operational safety.
How training builds competence and reduces risk
Competence, in the context of Legionella control, means three things: the ability to identify hazards before they become problems, the skill to operate control measures exactly as specified, and the confidence to escalate rapidly when something deviates from the expected range. Generic awareness courses tick a box but rarely achieve all three.

Training supports due diligence and legal defensibility by demonstrating that information, instruction, and training have been provided to every employee involved in the Legionella control scheme, including those carrying out monitoring or remediation. In the event of an outbreak or enforcement action, this documented training record is one of the most critical pieces of evidence you can produce.
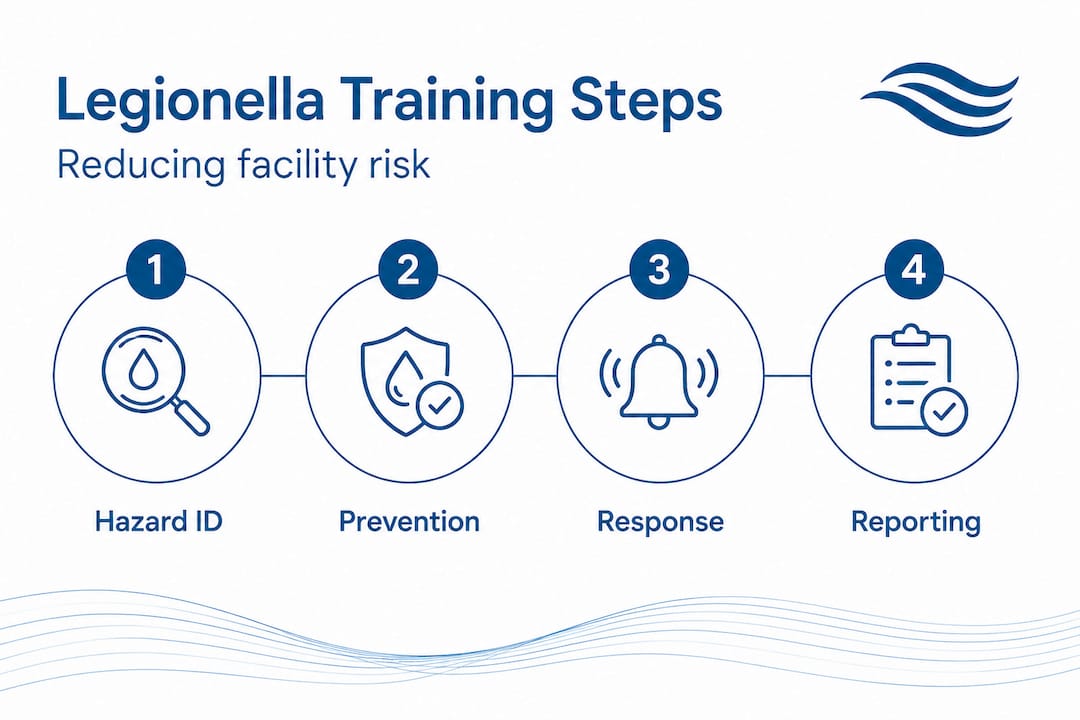
Here is how a structured training programme contributes to risk reduction at each stage:
Hazard identification. Staff learn to recognise the physical conditions that promote Legionella growth: dead legs in pipework, calorifiers operating below 60°C, infrequently used outlets, and poorly maintained cooling towers. They also learn where to look in their specific facility, not just in a generic diagram.
Control operation. Trained operatives understand not just what to do but why each control exists. A maintenance technician who understands why TMV outlet temperatures must be checked, rather than simply being told to complete the form, is far more likely to take an out-of-range reading seriously.
Deviation response. Staff learn defined escalation pathways: who to inform, what records to create, and what temporary control measures to apply while a fault is investigated. This stops minor deviations from becoming reportable incidents.
Post-change review. After any system modification, trained staff know to reassess whether existing controls remain adequate and to flag changes to the responsible person for a written scheme update.
Record integrity. Training reinforces why accurate, contemporaneous records matter legally and operationally. Staff who understand the purpose of documentation are far less likely to backfill logs.
Staff role | Core training outcomes |
Responsible person | Legal duties, scheme oversight, escalation authority, competency assessment of team |
Maintenance technician | Temperature monitoring, TMV servicing, system inspection, deviation reporting |
Cleaning and housekeeping | Outlet flushing, shower head cleaning, recognising visible biofilm or scaling |
Contractor and specialist | Site-specific induction, permit-to-work compliance, notification protocols |
Senior management | Strategic oversight, duty-holder responsibilities, resource allocation |
Pro Tip: Map every training requirement to a specific role and responsibility in your written scheme. Then set calendar reminders for refresher training that align with your system review cycle, not just an arbitrary annual date. When reviewing risk assessment competency, you should check whether each person named in the scheme has current, role-appropriate training to match their listed duties.
On large commercial or Legionella risk assessment sites, we regularly find that training records exist but do not map to the scheme. Someone is listed as responsible for monthly cooling tower checks, yet their training records show only a basic awareness course completed three years ago. That disconnect is a compliance gap, regardless of how tidy the paperwork looks.
Now that we understand training’s impact, it is vital to see how this approach is integrated in healthcare settings with high risk and regulatory scrutiny.
Training in healthcare: water safety management and role-specific frameworks
Healthcare facilities present a unique combination of vulnerable patients, complex water systems, and intensive regulatory oversight. HTM 04-01 does not treat training as a background requirement. It places structured, role-specific training at the heart of water safety management, tying it directly to risk identification, written scheme maintenance, and formal competency evaluations.
In healthcare settings, staff training is explicitly tied to structured water safety management involving risk identification, written scheme review, and competency evaluations, not simply to awareness raising. This means healthcare facilities managers cannot discharge their duty through a one-day group course. They need a programme that is documented, assessed, and linked to specific system responsibilities.
Key requirements for healthcare staff training include:
Water safety group membership training. The water safety group, which oversees the water safety plan for the site, must include members who are trained to interpret risk assessments, review control data, and make informed decisions about system changes.
Authorising engineer input. Larger NHS and independent healthcare sites are required to appoint an authorising engineer for water who provides independent technical oversight. This role carries specific training and experience requirements.
Competency-assessed roles. Technicians carrying out physical controls, such as temperature monitoring, shower head descaling, or calorifier inspections, must be demonstrably competent, with records showing what they were trained to do and when.
Patient-area specific awareness. Staff in clinical areas where immunocompromised patients are present, such as haematology or oncology wards, require additional awareness of the heightened risk profile and the enhanced controls in place.
Contractor management training. Those responsible for supervising contractors working on water systems must be trained to brief contractors on site-specific risks, issue permits to work, and verify that work has been completed to specification.
Pro Tip: Develop refresher training protocols that trigger automatically after any significant system change: a new wing opening, a period of reduced building occupancy, a major repair, or a change in water treatment supplier. Changes to the system mean changes to risk, and your team’s knowledge must keep pace. For detailed guidance on how healthcare water risk assessments should structure this, look at how competency assessment is embedded throughout the process rather than treated as a separate exercise.
With structured programmes in place, understanding how staff training helps prevent operational spikes and outbreak response is the next layer of practical knowledge.
Preventing edge cases and managing operational risk
Most written schemes anticipate normal operating conditions. They specify what to do when the building is occupied, the system is functioning, and staff are following routine procedures. What they rarely cover in sufficient detail are the edge cases: the situations where Legionella risk spikes because something unexpected has happened.
Training fills this gap. Specifically, it teaches staff to recognise when normal procedures are no longer adequate and to act before the risk escalates. Training helps prevent operational edge cases where Legionella risk spikes due to disturbance, stagnation, or aerosol generation, because staff learn the procedures and when to escalate or change controls.
Common edge cases that facilities teams encounter include:
System stagnation after reduced occupancy. A building that has been partially or fully unoccupied for several weeks, perhaps during a holiday period or a refurbishment, will have sections of pipework where water has been sitting at risk temperatures. Trained staff know to implement a recommissioning flushing procedure before normal use resumes, not simply to open the taps and hope.
Deep cleaning and maintenance disturbance. Descaling shower heads, opening calorifiers, or cleaning cooling towers all create aerosol and disturb biofilm. Without training, operatives may not appreciate that these activities temporarily elevate the risk and that enhanced controls, including personal protective equipment and post-work disinfection, are required.
System modifications and additions. A new branch of pipework, a replaced TMV, or a new outlet added to an existing ring main changes the hydraulic characteristics of the system. Trained staff know to flag these changes to the responsible person so the written scheme can be reviewed.
Unexpected temperature failures. If a calorifier fails to reach 60°C or a cold water tank is found to be above 20°C, trained staff know this is an immediate escalation event, not something to monitor quietly and note in the log.
When an incident does occur, the outbreak response steps your team should follow are:
Isolate the suspected source immediately and restrict access.
Notify the responsible person and, where required, the local authority or HSE under RIDDOR.
Collect water samples before any disinfection is carried out, preserving evidence for investigation.
Commission a specialist investigation and begin a root cause analysis.
Review and update the written scheme and training programme in light of findings.
Communicate transparently with affected parties, including building occupants and relevant health authorities.
For further context on how these controls integrate with formal written schemes, our method of works for compliance resource sets out the procedural expectations in detail.
Having established the operational benefits through training, let’s see what sets outstanding compliance teams apart and what is often missed in theory.
Hard-won lessons: the hidden value of practical, role-based training
After working across commercial, healthcare, and housing sites throughout the UK, one pattern is impossible to ignore. The facilities that consistently perform well in audits and avoid enforcement action are not necessarily the ones with the most detailed written schemes. They are the ones where every person named in the scheme actually knows what they are supposed to do.
Generic, one-size-fits-all training is one of the most persistent myths in water hygiene compliance. A group course that gives a caretaker, a ward manager, and a senior estates officer the same content is not training. It is awareness raising, and awareness alone does not change behaviour at the point of risk. The caretaker who understands flushing frequencies specific to their building will act differently from one who attended a generic half-day course three years ago.
What we have seen work well, again and again, is mapping training content directly to the responsibilities written into the control scheme. When a technician can point to a section of the written scheme and say “that is my job, and this is how I was trained to do it,” competence becomes visible and verifiable. That is exactly what ACOP L8 expects from a responsible person.
The second overlooked element is involving staff in scheme reviews. When operatives who carry out daily monitoring tasks participate in the annual review of the written scheme, two things happen. First, the scheme becomes more accurate because the people who know the system best contribute to it. Second, those staff develop a stronger sense of ownership over the controls they are responsible for. A real-world case study from one of our commercial sites illustrates exactly how this approach uncovered a dead leg that had not appeared in any previous assessment, simply because the maintenance operative was asked to walk the route with the assessor.
The uncomfortable truth is that most compliance failures are not failures of documentation. They are failures of communication, training, and accountability. Fix those, and the documentation takes care of itself.
Next steps: access expert Legionella training and support
Knowing what best practice looks like and building it into your organisation are two very different challenges. The detail required to train staff at the right level, for the right role, within a scheme that genuinely reflects your site, is considerable.
At Bespoke Compliance Solutions, we work with facilities managers and compliance officers across commercial and healthcare sectors to design and deliver bespoke Legionella training that is mapped to your site, your written scheme, and your team’s specific responsibilities. We also provide water testing and risk assessment services to ensure that your training programme is grounded in an accurate, current picture of your system’s risk profile. If you are ready to move from paper compliance to genuine operational control, we can help you get there.
Frequently asked questions
What legal requirements govern staff training for Legionella control in the UK?
Under ACOP L8, all staff involved in water hygiene or Legionella control must be adequately trained and competent to carry out their specific roles, with a competent responsible person overseeing the written scheme.
How often should staff receive refresher training for Legionella risk?
Refresher intervals depend on system complexity and any process or personnel changes; however, training should be paired with a competency framework that specifies frequency, assessment criteria, and triggers for after-change training.
What types of staff should be trained for Legionella prevention?
All staff with water system duties require role-appropriate training covering their specific responsibilities, whether they are the responsible person, a maintenance technician, or an operative carrying out routine flushing or monitoring.
Can training reduce liability in the event of a Legionella outbreak?
Yes. Structured training demonstrates due diligence and legal defensibility, particularly when staff roles and competency assessments are properly documented alongside training records.
Recommended
Comments