
Legionella in dialysis units: risks and controls
- Jun 2
- 9 min read

Legionella is a waterborne bacterium responsible for Legionnaires’ disease and Pontiac fever, transmitted primarily through inhalation of contaminated aerosol droplets from water systems. Dialysis units represent one of the highest-risk healthcare environments for Legionella proliferation, combining large daily water volumes with patients whose immune systems are severely compromised by kidney failure, diabetes, and comorbid conditions. Regulatory bodies including the CDC and CMS have issued specific guidance for healthcare water management precisely because the consequences of Legionella infection in patients are severe and frequently fatal. Understanding what Legionella is in dialysis units, how it spreads, and how to control it is not optional for facility managers. It is a clinical and compliance obligation.
What is Legionella in dialysis units and why does it matter?
Legionella pneumophila is the species responsible for the vast majority of clinical Legionella infections, and it thrives in the complex water distribution systems that dialysis units depend upon. Unlike most healthcare infection risks, Legionella spreads via inhalation of mist from contaminated water rather than through direct patient contact. This makes it a building infrastructure problem as much as a clinical one. Dialysis units are particularly exposed because haemodialysis requires each patient to be connected to a water-fed machine for three to five hours per session, several times per week. The sheer volume of water processed, combined with the plumbing complexity of a typical dialysis suite, creates multiple opportunities for bacterial colonisation and aerosol generation.
The term “Legionella risk in dialysis” is sometimes used narrowly to refer only to dialysate water quality. This is a critical misunderstanding. Legionella risk in a dialysis unit is a facility-wide water system issue, encompassing showers, handwashing outlets, ice machines, cooling towers, and any other water-fed device capable of producing aerosols. Facility managers who focus exclusively on dialysate purity while neglecting the broader building water system are leaving significant exposure unaddressed.
How does Legionella grow and spread in dialysis water systems?
Legionella colonises water systems when environmental conditions align to support bacterial growth. The key factors are well-established and directly relevant to dialysis unit infrastructure.
Temperature: Legionella grows between 20 and 45°C, with peak proliferation around 37°C. Hot water systems that fall below 60°C at the calorifier and cold water systems that rise above 20°C are both at risk.
Stagnation: Low-use pipework branches, dead legs, and infrequently flushed outlets allow water to sit and warm, creating ideal growth conditions. Dialysis units with seasonal fluctuations in patient numbers are particularly vulnerable during quieter periods.
Biofilm: Sediment and scale on pipe surfaces provide nutrients and physical protection for Legionella colonies. Biofilm allows bacteria to persist even when disinfectant residuals are present in the bulk water.
Disinfectant depletion: Chlorine residuals dissipate rapidly in warm, stagnant water or in systems with high surface area. Once residuals fall below effective levels, colonisation accelerates.
Aerosolisation: During dialysis treatment, water is processed through reverse osmosis units, storage tanks, and distribution loops before reaching the dialysis machine. Any point in this circuit that generates fine mist or spray creates an inhalation pathway for patients and staff.
Dialysis plumbing is inherently complex. Distribution loops, point-of-use filters, and multiple branch connections create hydraulic conditions that are difficult to manage without a detailed schematic and a structured maintenance schedule. Flushing low-use pipes is a basic but frequently overlooked control that directly reduces stagnation risk.
Pro Tip: Map every water outlet in your dialysis unit, including those not in regular clinical use, and assign each one a flushing frequency. Outlets used less than once per week should be flushed for at least two minutes, and the activity should be logged.

What are the risks of Legionella infection for dialysis patients?
Dialysis patients face a disproportionately high risk from Legionella infection compared to the general population. Kidney failure, diabetes, and the immunosuppressive effects of long-term dialysis treatment combine to create a patient group with severely limited capacity to fight respiratory infection. Infection outbreaks in haemodialysis units have caused confirmed cases of Legionnaires’ disease linked directly to contaminated water sources within the facility.
The clinical consequences are serious. Legionnaires’ disease presents as severe pneumonia requiring hospitalisation, and case fatality rates in immunocompromised patients are substantially higher than in the general population. Pontiac fever, the milder non-pneumonic form, causes flu-like symptoms but is rarely fatal. For dialysis patients, even a non-fatal Legionella infection can destabilise an already fragile clinical picture, leading to extended hospital stays and complications.
The operational implications for dialysis units are equally significant. A confirmed Legionella case linked to a facility triggers a mandatory investigation, potential suspension of services, and regulatory scrutiny from CMS and local public health authorities. Haemodialysis exposes patients to 120 to 180 litres of treated water per session, which means that water quality failures are not isolated incidents. They affect every patient treated during the period of contamination. Compliance with AAMI RD52 water quality standards and CMS Conditions for Coverage is not merely a regulatory formality. It is the operational framework that keeps patients safe and facilities open.
The following sequence describes how a Legionella exposure event typically escalates in a dialysis setting:
Stagnation or temperature failure creates conditions for bacterial growth in a section of the water system.
Legionella colonises biofilm within pipework or storage tanks, often without visible signs.
Aerosols generated during treatment or routine water use carry bacteria to the breathing zone of patients and staff.
A patient develops pneumonia. Clinical teams may not immediately suspect Legionella, delaying diagnosis.
Retrospective water testing confirms contamination. Regulatory notification and facility investigation follow.
The unit faces service disruption, reputational damage, and potential enforcement action.
Understanding this sequence is the basis for managing Legionella risk in immunocompromised patients before an incident occurs rather than responding to one.
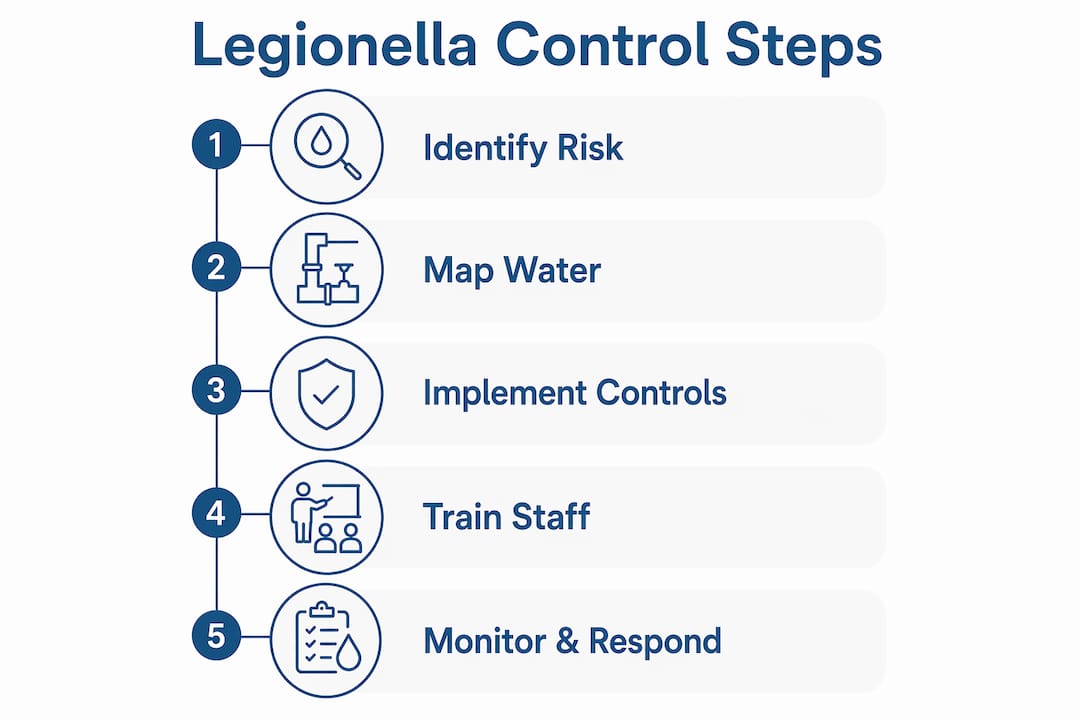
What prevention and control strategies work for dialysis units?
Preventing Legionella in healthcare settings requires a structured, documented Water Management Programme. Since 2018, CMS requires healthcare facilities to implement Water Management Programmes guided by ASHRAE 188 and CDC toolkit frameworks. A Water Management Programme is not a single document. It is an operational system that integrates engineering controls, monitoring protocols, staff responsibilities, and corrective action procedures.
Control measure | Purpose | Frequency |
Hot water temperature checks | Maintain storage above 60°C to inhibit Legionella growth | Weekly minimum |
Cold water temperature checks | Confirm cold supplies remain below 20°C | Weekly minimum |
Outlet flushing | Prevent stagnation in low-use branches | Weekly for low-use outlets |
Chlorine dioxide dosing | Secondary disinfection to suppress colonisation | Continuous or periodic per system design |
Water sampling and culture | Confirm microbiological control and detect colonisation | Monthly or per AAMI RD52 schedule |
Risk assessment review | Identify new hazards from system changes or usage patterns | Annually and after significant changes |
Secondary disinfection is a particularly important tool in dialysis settings. A 23-year hospital study demonstrated that iterative chlorine dioxide treatments reduced Legionella positivity from above 50% to below 1% over the study period. This finding underlines a critical principle: single interventions rarely achieve lasting control. Sustained, layered approaches combining chemical treatment, physical remediation, and system redesign are required.
Physical infrastructure improvements matter as much as chemical controls. Dead legs should be removed or capped. Thermostatic mixing valves require regular servicing to prevent them from becoming colonisation points. Point-of-use filters provide a last line of defence at high-risk outlets but are not a substitute for system-wide control.
Pro Tip: When commissioning a new dialysis suite or refurbishing an existing one, involve your water hygiene specialist before construction is complete. Retrospective removal of dead legs and poorly designed pipework is significantly more disruptive and costly than designing them out at the build stage.
Staff training is a non-negotiable component of any effective control programme. Clinical and facilities staff need to recognise the signs of water system failure, understand their responsibilities within the Water Management Programme, and know how to escalate concerns. Legionella awareness training aligned with HSE L8 guidance provides the foundation for a competent, responsive team.
How to monitor and respond to Legionella detection in dialysis water
Routine monitoring is the mechanism by which a Water Management Programme moves from paper to practice. CMS Conditions for Coverage and AAMI RD52 set the water quality standards and documentation protocols that dialysis units must meet. Testing schedules should cover microbial counts, endotoxin levels, and chemical parameters at defined intervals, with results logged against pre-agreed action levels.
Effective monitoring in a dialysis unit covers the following areas:
Dialysate water quality: Microbial and endotoxin testing per AAMI RD52 at the frequency specified by the standard and the unit’s own risk assessment.
Hot and cold water distribution: Temperature monitoring at sentinel outlets and representative points throughout the system, with automated logging where possible.
Legionella culture testing: Periodic sampling from high-risk points including calorifiers, cooling towers, showerheads, and any outlets serving immunocompromised patients.
Disinfectant residuals: Regular measurement of chlorine or alternative disinfectant levels to confirm ongoing efficacy.
Corrective action records: Every exceedance of an action level must be documented alongside the response taken and the outcome achieved.
When Legionella is detected, the response must be immediate and structured. Monitoring indicating Legionella presence should trigger a multidisciplinary response involving infection control, facilities management, clinical leadership, and an external water hygiene specialist. The response sequence should include confirmation sampling, immediate risk assessment, implementation of secondary disinfection, and communication to relevant stakeholders including the local health protection team.
Automated temperature monitoring systems remove the reliance on manual checks and provide a continuous audit trail. For dialysis units managing multiple water outlets across a large facility, automated systems reduce the administrative burden on facilities staff while improving the reliability of the compliance record. Digital logbook systems that capture test results, corrective actions, and maintenance activities in real time are increasingly the standard expected by CMS and CQC inspectors.
Key takeaways
Effective Legionella control in dialysis units requires a facility-wide Water Management Programme combining temperature control, secondary disinfection, routine monitoring, and trained staff, not dialysate management alone.
Point | Details |
Facility-wide risk | Legionella risk extends beyond dialysate water to all water outlets capable of generating aerosols. |
Growth conditions | Temperatures between 20 and 45°C, stagnation, and biofilm are the primary drivers of colonisation. |
Patient vulnerability | Dialysis patients face significantly elevated risk of fatal Legionnaires’ disease due to compromised immunity. |
Regulatory obligation | CMS and AAMI RD52 mandate documented Water Management Programmes and defined testing schedules. |
Iterative control | Sustained secondary disinfection combined with physical infrastructure improvements achieves lasting bacterial suppression. |
Why the building matters more than the machine
One pattern I see repeatedly when working with dialysis facilities is the assumption that Legionella risk begins and ends with the dialysis water treatment train. The reverse osmosis unit, the storage tank, the distribution loop: these receive meticulous attention, as they should. But the showers in the patient changing area, the handwashing sinks in the treatment room, the infrequently used utility outlets at the end of a corridor: these are often invisible to the water safety plan.
Legionella does not respect clinical boundaries. A colonised showerhead in a patient bathroom adjacent to a treatment bay is as much a risk as a contaminated water loop. The aerosol does not know it is outside the dialysis circuit. What I have found in practice is that the facilities and clinical teams in dialysis units often operate in parallel rather than together. The clinical team manages dialysate quality. The facilities team manages the building. Neither group has full sight of the whole system. The most effective Legionella control programmes I have seen are those where a single Water Management Programme covers both domains, with clear ownership, shared documentation, and regular joint review.
The NHS GP surgery outbreaks documented in recent years reinforce this point. In almost every case, the contamination source was a part of the building water system that sat outside the primary clinical focus. Dialysis units should take that lesson seriously.
— Sammi
Legionella compliance support for dialysis facilities
Bespokecompliancesolutions works with healthcare facilities across the UK to build and maintain Legionella compliance programmes that are specific to the demands of clinical water systems. For dialysis units, that means going beyond generic water hygiene advice to address the precise risks created by high-volume water use, complex plumbing, and a patient population that cannot afford a water safety failure.
From water system disinfection and Legionella water testing to automated temperature monitoring and bespoke logbook systems, Bespokecompliancesolutions provides the full range of services needed to achieve and maintain compliance with CMS, AAMI, and HSE L8 requirements. Contact the team to discuss a compliance programme tailored to your dialysis unit.
FAQ
What is Legionella and why is it a risk in dialysis units?
Legionella is a waterborne bacterium that causes Legionnaires’ disease through inhalation of contaminated aerosols. Dialysis units are high-risk environments because they process large volumes of water daily and serve patients with severely weakened immune systems.
How does Legionella get into dialysis water systems?
Legionella colonises water systems where temperatures fall between 20 and 45°C, stagnation occurs, or biofilm is present. Dead legs, low-use outlets, and poorly maintained storage tanks are common colonisation points in dialysis facilities.
What regulations govern Legionella control in dialysis settings?
CMS Conditions for Coverage require healthcare facilities to implement documented Water Management Programmes, while AAMI RD52 sets specific water quality standards for dialysis water. Both frameworks mandate routine testing, corrective action procedures, and staff training.
How often should dialysis units test for Legionella?
Testing frequency should follow AAMI RD52 schedules for dialysate water quality and the facility’s own Water Management Programme for the broader building water system. High-risk outlets serving immunocompromised patients warrant more frequent sampling than standard clinical areas.
Can Legionella be eliminated from a dialysis water system?
Legionella colonisation can be suppressed to very low levels through sustained secondary disinfection, physical infrastructure improvements, and rigorous monitoring. Research shows that iterative chlorine dioxide treatment reduced hospital water system positivity from above 50% to below 1% over a 23-year period, demonstrating that lasting control is achievable with consistent effort.
Recommended
Comments